Saira, PA in General Surgery & Research

Saira Rashid is a Physician Assistant working in General Surgery at Mount Sinai Hospital. She completed her Bachelor’s of Science in Human Biology at University of Toronto and went on to complete her PA degree at McMaster University in 2012. Along with clinical practice, Saira has completed several quality improvement projects at Mount Sinai and plays an active role in training residents and students. Her interests are doing research work and advocating for the PA profession.
Her research work has been recognized at the annual PA conference for the last four years including winning 2nd place in the CPAEA poster sessions in 2015 and winning 1st place in 2014, 2016-2018. Her most recent submission has been on “Randomized controlled trial on a PA led discharge monitoring tool following colorectal surgery”. She has trained PA clerks and acts as a facilitator for the UOFT PA program.
Working as a Surgical PA
Did you know you would be working in surgery as a second-year PA student?
I did not know I would be working in surgery as a second year PA student.
While I was going through my clinical rotations, I kept an open mind about what to expect. I wanted to learn as much as possible from the different rotations I was completing. It was closer to the end of second year that I gathered my thoughts about what I enjoyed the most.
I really liked internal medicine because of clinical acuity of the patients. I also liked the practical hands on skills that I gained through my Emergency Medicine and Family Medicine rotations (e.g. suture lacerations, incision and drainage, etc.).
So when it was the time to apply for jobs, I realized surgery was a good fit for me because it offered a bit of both: the acute medical care on the inpatient ward and a hands on practical component such as assisting in the operating room or performing procedures on the ward like wound care, ostomy care etc.’
What is a typical day and week in the life of a PA in surgery?
On a daily basis I am involved in managing the inpatient ward. This wasn’t the case when we were initially hired but now with the establishment of medical directives, which are very comprehensive, I’m able to manage the inpatient ward with minimal assistance from the residents. On an ongoing basis I round on inpatients with surgical residents, liaise with nurses and the allied health care team for care plans and disposition.
If I were to look at my schedule on a weekly basis, I have two OR days, I am either a first or second surgical assist. I assist in prepping, draping, opening and closing for laparotomies and assisting throughout the case in providing exposure and hemostasis.
Two days per week are outpatient clinic days. I see consults alongside the residents, and review with staff.
One day a week is a catch up day. I free up a few hours to work on various research and academic projects that I am currently working on.
Has your scope of practice changed since gaining experience?
It sure has. When I started at Mount Sinai Hospital in 2012, I wasn’t sure what the expectations were. My supervising physicians were very supportive and wanted to see the profession grow, but it would take some time before the PAs would establish a niche, per say in general surgery.
Looking back to the five years that I’ve been working at Mount Sinai Hospital, I see my role as having three tiers:
Clinical
Academic
Research
The clinical aspect of my job I’ve touched on previously.
Second is academic. I am very passionate about teaching PA students, medical students and even some of the residents. Now that I’ve been working as a general surgery PA for several years, I’ve gained competency in managing general surgery patients. I am also aware of different physicians’ preferences for various management plans. Hence, I am able to guide junior surgery residents in inpatient perioperative care, management of certain postoperative complications and advise on preferred clinical frameworks.
The last piece is research. Working with physicians that are highly research-driven, I’m able to take on many interesting research projects. Of date, I have completed several quality improvement projects that have had huge impacts on patient care in our department.
Any tips for PA students aspiring to work in surgery?
I think students should have an open mind about their interests as they complete PA school. If they like surgery and the environment, I would recommend that students do an elective rotation in a surgical speciality of interest. Preferentially, in a place that is accepting of PAs so that you can get a feel for what the profession would look like and how the scope of practice could be broadened in that particular place. [at the top of your scope of practice].
Conducting Research as a Surgical PA
My interest in Research
My interest in research is around health promotion. I believe PAs play an important role in being patient advocates, and health advocates essentially. As practicing PAs, I know many of us face current processes and clinical frameworks in our workplaces that can be modified to help improve patient outcomes. I think PAs are highly capable of identifying those opportunities for improvement and working to enhance quality of patient care.
Personally, I’m always looking for opportunities and ways to improve patient safety and quality of care that I deliver. Overall, a lot of the projects that I’ve done to date are around quality improvement. I’ll talk about the two that our group is currently working on right now.
Research Project 1: PA led patient discharge app for Colorectal Surgery
For the colorectal surgery patients, we have developed a mobile app as a discharge monitoring tool, to support postoperative patients after they’ve been discharged from the hospital.

Saira & Alifiya presenting at the PA Poster Presentation on the mobile app.
There’s compelling evidence that postoperative patients are unsure of discharge instructions as they transition from hospital to home. Patients have a lot of questions and uncertainties about what is normal vs. abnormal course of recovery at home. In particular, colorectal surgery patients are very anxious about their complex care needs at home, namely incision, drain and stoma care.
Hence, we’ve developed a discharge mobile app, a monitoring system that essentially checks in virtually with patients once they are home. Inside this free app, we’ve developed a survey, called the “daily health check”, based on a validated score, quality of recovery-15 (QOR-15). In patient-friendly language, the survey asks some of the similar questions we would ask to inpatients. Questions that include: How’s your pain on a scale of 1-10? Do you have nausea? Are you able to eat? Do you have any issues around your incisions? Any problems with the drain or Stoma?” and so on. It is a pretty comprehensive questionnaire. The app also features the ability to take a picture of a concerned wound or stoma.
Patients fill out the survey every day that they’re home for the first fourteen days. If everything is okay, then the patients get a satisfactory progress report at the completion of the survey with some helpful tips and education material. However, if patients’ responses raised red flag symptoms (such as fever, wound complication, ostomy issues, intestinal blockage), then the patients are queued to expect a “call back” from the PA or instructed to go to the ER for severe problems.
On an encrypted provider web dashboard, I look at the patients’ answers to the surveys. For all the “call back” statuses, I follow up with patients with a phone call within one business day, resulting in counselling over the phone or arranging for an urgent clinic appointment. In doing so, patients can bypass the emergency department, where they’d have to wait several hours perhaps to be seen for a relatively minor issue.
For this project, we completed a pilot study which showed that patients loved being able to connect with the a member of the surgical team who knows their medical and surgical course quite well and can provide useful follow up.
Right now, we are completing a randomized control trial, which we’re very excited about! We’re almost close to the end and anticipate promising results, namely improving patient outcomes and reduced bounce back to the ER and hospital readmissions.

Research Project 2: Jackson Pratt drain device for Breast Surgery patients
This is a very exciting project for our Breast Surgery patients.
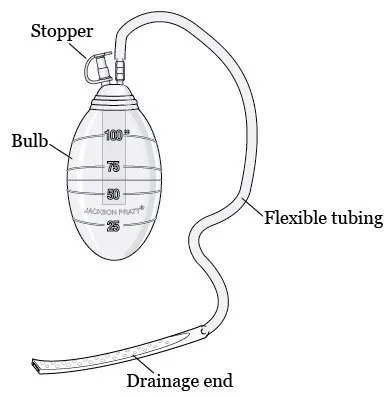
A Jackson-Pratt Drainage System Image from: MSKCC.org
A little bit of background: most of our breast surgery patients, especially those that undergo mastectomies and/or axillary node dissections have a Jackson Pratt (JP) drain placed under the incision. The purpose of the drain is essentially to evacuate fluid that builds up under the incision as part of healing so to prevent any seromas or hematomas that may lead to wound complications.
It’s our clinical impression that a lot of post-operative breast surgery patients return to ER or FD for JP malfunction (i.e. blocked drainage tube, increased incisional pain, swelling and/or erythema, discharge around the drain tube or the incision). These unexpected symptoms cause considerable amount of anxiety in patients and they seek medical attention to be reassessed. Occasionally, increased seroma and hematomas lead to wound breakdown, requiring a prolonged wound closure by secondary intention.
In an attempt to improve patient outcomes for aforementioned drain related problems, we are introducing a JP drain evacuation device. It is essentially a small plastic device that anchors onto the drain tubing at the insertion point and by sliding the device down the tubing, it strips the drain clean of any debris or clot. By introducing this JP-clearing device for post-op use, we hope to evacuate any seromas or hematomas from building up under the breast incision. As a result, we hope to prevent wound-related complications, improve patient outcomes, quality of care and decrease wound related unscheduled visits to the ER or the family physician.
This intervention has shown to work in other settings. So far it’s too early to say what we’ve accomplished. However, with randomization, where some patients receive the JP-clearing device and others do not, we are hoping to have compelling results in the end.
What do you enjoy about research?
Challenging: I enjoy research because it’s challenging and exciting at the same time. Thinking outside the box, problem solving around an idea that I am particularly excited about and then designing and executing the project, is stimulating for me
Benefits patients: Over time, I’ve built research into my PA role at Mount Sinai. I enjoy seeing that patients benefit from the ideas I’ve brought to the table and the processes and clinical frameworks that have improved as a result of my research work.
Fulfilling: My work is often appreciated by both patients and staff for the positive contribution to quality of care, so that’s very gratifying. Also, being able to share the knowledge and research work with my peers at the annual CAPA conferences is very fulfilling. For the last several years, our group at MSH has been recognized for the research work that we’ve done, winning 1st place prize for original research in poster presentations, which is very encouraging.
What are the benefits of conducting research as a PA?
There are many benefits for conducting research.
Professional leaders: I believe research is the platform whereby leaders in medicine communicate their ideas, inventions, evidence-based guidelines, supporting or disapproving certain ideas etc. So, if PAs conduct and publish their research work, they become leaders in medicine sharing their expertise and highlighting the value they add to the healthcare system.
Challenges status-quo: Another benefit, especially of health promotion research projects, is that it challenges the status quo. Humans, being creatures of habit by nature combined with bureaucracy of often large healthcare organization, it can make difficult to advocate for improving existing patient care. However, as health care advocates, I think PAs can play a vital role in illustrating the need for health promotion as a result of their research work.
Also, in the grand scheme of things the PA profession is fairly new. The more research PAs conduct and publish, the more value we are able to show, advocating for our profession. So, when our PA representatives go to negotiation meetings with those in charge about regulation and accreditation of our profession, it would help tremendously to show the value that PAs have added in many different settings in the Canadian healthcare system.
If more and more PAs publish their research work demonstrating value as a PA in a particular setting,– it speaks volumes to what we’re able to do, collectively, as health care professionals.
What are you changing in your practice as a result of the research you’ve done?
Some of the research projects that I’ve completed, have actually modified the delivery of patient care on our surgical floors. I’ll discuss one example in particular.
Standardized home care pathways- We know there’s strong evidence that unclear communication regarding discharge planning makes it difficult for patients to transition from hospital to home, compromising patient safety.
We noticed that our postoperative breast surgery patients often required home care referrals for routine interventions such as drain and incision care. Since these referrals were completed online by residents rotating frequently, the parameters of care written in the referrals varied. As a result, following problems were identified:
Referrals often lacked necessary information compromising patient care at home
Incomplete referrals required a resident to amend referral, delaying patient discharge
Residents found it very time consuming to type out referrals for routine interventions daily
To address these issues, I created a CCAC template with parameters of care for routine intervention (i.e. JP drain care) that was comprehensive, with all the necessary detail. This template was approved by the staff surgeons, nurses and home care coordinator. Upon approval, the templates were made available on the TCLHIN home care referral portal. With just one click, the template and the entire care pathway would be auto-populated to the referral.
Since the implementation of this tool, there has been drastic reduction in the number of queries regarding referral completion. This also improved the process of discharging patients as the referrals no longer delayed discharges. The residents also benefited tremendously from having pre-approved templates as they could complete referrals in seconds with all the necessary details.
Most importantly, patient care was improved since there was no miscommunication about the care they should receive at home.
That’s just one example of what I was able to do successfully and how it’s actually implemented in my day to day practice.
How do you balance your work and research with clinical responsibilities?
So that’s very challenging. It goes without saying that I am wearing many hats throughout the day. The residents see me as a vital member of the surgical team. Appreciating my clinical role, they are not necessarily aware of my non-clinical duties such as academic and research. So it’s very difficult to balance my duties and find time for my research work.
I’m fortunate to be working with a group of physicians that support my research work and are able to advocate for me to say “Saira needs a few hours set aside where she’s going to catch up some of her projects” and that’s my protected time.
What challenges did you encounter in the beginning of starting research?
I don’t come from a research background. At the very beginning I was very uncertain and fearful because I felt I had no sense of direction – I didn’t know where to begin. I did volunteer for small research projects when I was doing my undergraduate degree, but in PA school, it was such a condensed medical curriculum that I couldn’t free up enough time to delve into research at that point.
That uncertainty was challenging to overcome. I’m fortunate to be working with a group that has very strong research leaders and they’ve supported my ideas, providing constructive feedback and mentoring me along the way.
I encountered early on that we had a research group that consisted of research coordinators and statisticians within the hospital that could help. I can see that could be challenging for beginners to research if they do not have access to these resources. Other challenges can be really getting buy in for your project and finding collaborators. Sometimes finance is an issue, and grants can be difficult to get. However Mount Sinai has a great research group, and we were able to push for ideas and get funding.
How to Do Research
What is your research process from initiation to publication?
I have a little bit of an algorithm on how I like to do things or how I like to approach research projects.
Step1: Identify the Topic
The first step is identifying what the research topic for our study.
Most of my projects are Quality Improvement (QI) projects.
Step 2: Gather Background Information
The next step is to gather background information, which could involve: looking at baseline data that you’d like to use as control, doing a literature review to see what other similar studies are published, reviewing evidence to see if the topic of interest is worth researching.
Gathering data can be difficult, especially if you’re working in a hospital and you don’t know how to approach it – there may be challenges in getting access to raw Electronic Medical Records (EMR) data that might otherwise be more accessible in other settings.
Step 3: Brainstorm Ideas
You are asking yourself, “How do I want to approach the issue at hand? How can different studies be designed? What’s the most efficient, practical or pragmatic way to approach this question / topic?”
Tip: Identify Stakeholders!
It’s important to also identify stakeholders and/or key players that may need to get involved in your research
Do you have patients involved? If so you may require research ethics board approval
Are you doing chart review? Who do you have to go through to get the charts, and permission to review the charts?
Identifying the key players in your research will help you navigate and come up with a research working group, and who it is that you need to include in your research meetings to help you move your ideas forward.
Step 4: Design the Study Protocol
Once I have done the background work, I have a rough idea of the process, and I know the people that are involved, then I design the study protocol.
In the study protocol, I am very clear about the thesis, the main goal. Here you clearly state methods, study outcomes, anticipated results, so you have a reference frame to go back. This is helpful when you get too bogged down with actually collecting the data and doing the research, you may lose track of the bigger picture.
Tip: Create a Data Abstraction Form
A Data abstraction form is a way of collecting all of your raw data so its encrypted/protected if there is patient information. It’s also a central tool or master sheet where you can plot your raw data that you will analyze later on.
If you have all of your tools in place first, it makes it easier to carry out the research once you’re actually doing the project.
Step 5: Execute the Project
This is where you are actually doing the project
Step 6: Publishing the project
Once you finish the project and you can look at your results and drawn some conclusions, you choose a format to present the data. You can choose to present it as a written paper, or a poster presentation.
How can beginners get started with research?
Look at the PA role itself. If we dissect the role, there are some really good research ideas you can get from there.
PA Research through Increasing Health Care Access
For example, we know that PAs increase access to health care in primary care through:
Reduced wait times
Reduced physician burnout
Increased number of patients seen in clinic
If we even look at some of those and dissect that, we can design a research project around that topic – which is very valuable!
To take this example further, let’s say you reduce wait times as a PA in primary care, you can gather data, keeping track of the patients you see. This data can be compared to baseline data in the EMR you may have against wait times BEFORE a PA was added to that practice.
This topic of reducing wait times is a pretty solid research project, and it speaks volumes because once you publish it, you’re able to show the value you added to that particular setting.
PA Research through Clinic Workflow
Some of the ways existing PAs can get into research would be from looking at their current workflow in a clinical setting. For example, we all face moments where we say, “Gee, I wish I could make this better” or “if this framework could be modified, it could really improve patient outcomes” while we’re working in clinic, in the operating room or on the wards.
Workflow issues are typically problems we face in everyday practice. I think if we capitalize on those ideas, they can yield pretty good research projects.
An example of a research idea that came from Surgery / Patient Care workflow:
For example, going back to my current project we’re doing for our breast surgery patients, we realized that a lot of these women were already very anxious about their diagnosis having just had surgery. They were worried about drains working improperly, increased pain and swelling.
For me as a PA clinician, that was an ‘aha’ moment to say, “I wish I could change that for them” or “given everything they’ve gone through with chemotherapy, radiation and surgery, I wish they wouldn’t have to suffer with the drain related minor issue at home”.
So capitalizing on that, we designed a project. This required collaborating with my coworkers and physicians.
How can PA students incorporate research during PA school?
There are a number of ways PA students can get involved in research. One may include an opportunity through a supervising physician/PA in the clerkship to volunteer or participate in their existing research projects. It’s a great way to get your foot in the door and to see how research is conducting, vicariously.
For someone like me who does not have a research background, that sense of fear or uncertainty might be lifted once you’ve seen a research project or trial being performed.
It can also make you feel more confident and motivated once you are a practicing PA.
Also staying up to date with the PA literature via JAAPA and JcanPA, students can learn about various research opportunities and get inspired to conduct their own research projects.
Journal of Canada’s PAs (JCanPA.ca), is a great platform where student PAs can publish research and get valuable feedback.
Is there a lot of research about PAs in Canada right now?
There is not, but I’m confident and optimistic that it’s emerging. Conducting research is not built into the PA training, in the Ontario schools. I think there is value in PAs understanding and learning the importance of research, and what it means for our profession from the PA training programs.
We’re definitely on the path to having more research and publications coming from PAs, especially since the establishment of the JCANPA, an open access journal for Canadian PAs. I believe PAs are highly competent individuals, with a lot to offer. I am optimistic that more research is coming down the pipeline.
What are your future directions in research?
I’m always open and always looking for ideas and opportunities to improve the current health care system and processes. I’m going to continue researching and publishing more, and writing for more PA journals. I’m hoping to bring new projects and new ideas to the Canadian PA conference next year!